Sunday, February 13, 2005
Using Passwords? Switch to Pass-phrases, Instead.
-
Printer Friendly|#| Trackback
Slashdot points to a very interesting blog entry by a Microsoft engineer in which he makes it perfectly clear how single
passwords are not secure any longer:
" So with all of these highly successful, highly effective attacks on passwords (dictionary attacks, brute-force attacks, pre-computation attacks) I've come to the conclusion that there is simply too much risk associated with passwords and that users of Windows should simply stop using them to avoid this risk. "
Instead, he recommends pass-phrases:
" Pass-phrase LENGTH, not complexity defeats these attacks. Short, but complex passwords should be shunned as they are not truly secure anymore and you are deceiving yourself if you think they are. Long pass-phrases (14 characters or more) are the future (along with 2-factor or more authN, but that's another blog for another day) and are the only way to go if you want to ensure that you won't get hacked via any type of password based attack of any kind. "
Think CPAP Mask After Major Abdominal Surgery
-
Printer Friendly|#| Trackback
JAMA just published Continuous positive airway pressure for treatment of postoperative hypoxemia: a randomized controlled trial and those of us giving anesthesia for open major abdominal surgery should take note. Here's the abstract:
" Results Patients who received oxygen plus continuous positive airway pressure had a lower intubation rate (1% vs 10%; P = .005; relative risk [RR], 0.099; 95% confidence interval [CI], 0.01-0.76) and had a lower occurrence rate of pneumonia (2% vs 10%, RR, 0.19; 95% CI, 0.04-0.88; P = .02), infection (3% vs 10%, RR, 0.27; 95% CI, 0.07-0.94; P = .03), and sepsis (2% vs 9%; RR, 0.22; 95% CI, 0.04-0.99; P = .03) than did patients treated with oxygen alone. Patients who received oxygen plus continuous positive airway pressure also spent fewer mean (SD) days in the intensive care unit (1.4 [1.6] vs 2.6 [4.2], P = .09) than patients treated with oxygen alone. The treatments did not affect the mean (SD) days that patients spent in the hospital (15 [13] vs 17 [15], respectively; P = .10). None of those treated with oxygen plus continuous positive airway pressure died in the hospital while 3 deaths occurred among those treated with oxygen alone (P = .12). "
I remember the first time someone suggested using CPAP for the struggling patient in the recovery room after major abdominal surgery. I snorted and mumbled something under my breath about how the patient needed an endotracheal tube and should have taken the offered thoracic epidural. I went back to bed, convinced that I'd be called in an hour or two to intubate the patient who would by then certainly be in extremis. You know what? They never called me that night and this paper helps me understand why.
I think I need to modify my internal algorithm for post-anesthesia management of these often difficult cases to reflect the option of CPAP as a middle ground between mask oxygen and endotracheal intubation.
Screening for AAA Recommended for Smokers Aged 65-75
-
Printer Friendly|#| Trackback
The U.S. Preventive Services Task Force (part of AHRQ) now 'recommends one-time screening for abdominal aortic aneurysm (AAA) by ultrasonography in men aged 65 to 75 who have ever smoked.'
" Rationale: The USPSTF found good evidence that screening for AAA and surgical repair of large AAAs (5.5 cm or more) in men aged 65 to 75 who have ever smoked (current and former smokers) leads to decreased AAA-specific mortality. There is good evidence that abdominal ultrasonography, performed in a setting with adequate quality assurance (i.e., in an accredited facility with credentialed technologists), is an accurate screening test for AAA. There is also good evidence of important harms of screening and early treatment, including an increased number of surgeries with associated clinically-significant morbidity and mortality, and short-term psychological harms. Based on the moderate magnitude of net benefit, the USPSTF concluded that the benefits of screening for AAA in men aged 65 to 75 who have ever smoked outweigh the harms. "
Patients should also be made aware that there is an alternative to open AAA repairs known as 'endovascular repair.' NEJM recently published A Randomized Trial Comparing Conventional and Endovascular Repair of Abdominal Aortic Aneurysms which concluded:
" On the basis of the overall results of this trial, endovascular repair is preferable to open repair in patients who have an abdominal aortic aneurysm that is at least 5 cm in diameter. Long-term follow-up is needed to determine whether this advantage is sustained. "
As an aside, wouldn't it be nice to be able to query our electronic medical record for all patients in our primary care practice who meet this criteria? Oh wait. We don't have EMR's (for the most part).
Saturday, February 12, 2005
Citation Classics in Anesthetic Journals
-
Printer Friendly|#| Trackback
I was listening to some friends talk about taking a large set of information and making it more useful to the user when I thought about a project I helped with to try to remedy this with regard to the body of published literature in medicine. PubMed is the National Library of Medicine's big online database of medical articles (no, I didn't help with that). Searching for a term on PubMed usually gets lots of results but doesn't necessarily get you any closer to finding that key reference that people consider the classic or definitive paper in the field.
As a teacher in academic anesthesia, I saw residents (note the past tense) had little hope of finding the 'right' paper to read unless I gave it to them. If I said 'read about airway management' they would no doubt find some things about airway management, but probably not the paper on airway management. Unless of course they were able to search a subset of articles in PubMed defined in advance to be especially relevant to their field of study. That's how we conceived of the idea of 'Key References'--make it easy to assemble a list of references for whatever purpose. To make it easy, we used a unique identifier for each article called the PubMed ID Number (PMID). Seth Dillingham then wrote a plugin for Conversant that could take that PMID and go to the PubMed system and (politely) request information about the reference such as title, authors, citation, and even the abstract.
'Citation classics in anesthetic journals' by Baltussen and Kindler is comprised of 'seminal advances in anesthesia' which give 'a historic perspective on the scientific progress of this specialty'. The advantage of having them available online as a compilation lies in the fact that they 1) are searchable and 2) linked to related articles in PubMed (something which even the online version of the original article even does not do).
See for yourself: Citation Classics in Anesthetic Journals
After looking up all 100 PMID's for these articles I wrote to the journal editors and suggested they require authors to include PMID's for references they cite in each article but (apparently) failed to make a convincing enough case. Sort of like in, oh, 1995 when I suggested to the editors of another journal that they could put their articles online using Highwire Press and was told that they had their hands full putting back issues on CD.
Thursday, February 10, 2005
Coming To A School Near You: Super Size Me
-
Printer Friendly|#| Trackback
" What happens when a man eats nothing but McDonald's food for 30 days? It's a lesson that schoolchildren across the country are about to find out.
Morgan Spurlock, director and star of "Super Size Me: A film of epic proportions," is releasing an edited version of the film for classrooms. The school version of the Academy-Award nominated film is scheduled to be released after the Feb. 27 Oscars (news - web sites) ceremony. "
Um. Can we show it in hospital waiting rooms?
[via Yahoo News]
"What the Doctor Saw"
-
Printer Friendly|#| Trackback
Published in the Fulton County (Georgia) Daily Report: What the Doctor Saw:--The court system through the eyes of a surgeon sued for malpractice (PDF--432k)
" Outstandingly reported account of a surgeon's professional liability trial from the standpoint of the defendant and his family as well as the lawyers on both sides. "
[Via Overlawyered]
Does it really cost 800 million dollars to develop a new pill?
-
Printer Friendly|#| Trackback
Estimating the Costs of New Drug Development: Is it really $802m?:
" Abstract:
This paper replicates DiMasi et al (2003) drug development cost estimates using their published survey cost estimates along with information from a publicly available data set. The results suggest that the expected cost of developing the average drug is even higher than the DiMasi et al (2003) estimate of $802m (in 2000 dollars). The paper estimates the capitalized out-of-pocket cost per new drug to be between $839m and $868m (in 2000 dollars). The paper similarly estimates the expected cost of the average new drug with certain characteristics such as primary indication. It is shown that the expected cost of developing the average HIV/AIDS drug is $479m, while the expected cost of developing the average rheumatoid arthritis drug is twice that, at $936m.
...[continues]..." "
PDF (184k)
[Via Marginal Revolution]
Tuesday, February 8, 2005
I want a Bluetooth pre-tracheal stethoscope
-
Printer Friendly|#| Trackback
During my anesthesiology training, attendings encouraged me to use a pre-tracheal stethoscope--basically a metal bell that rested on the base of the patient's neck over the trachea which could be used to listen to breath sounds during general anesthesia. This usually involved a hollow tube running from the stethoscope to an earpiece in the anesthetists ear. FM transmitter were available for wireless monitoring.
I still think this is usefull, especially for cases using a laryngeal mask airway (LMA). Trouble with an LMA is usually preceded by 'crowing'--a high pitched noise caused by the passage of air over partially closed vocal cords. This can progress to frank laryngospasm, airway obstruction, and the generation of very large negative intra-thoracic pressures and negative pressure pulmonary edema.
What would the modern equivalent be like? Bluetooth transmitter. Wireless ear phone. I wonder if I can do this with my PowerBook somehow? I'd need a box to convert the sound from the stethoscope to a digital signal (and amplify it), then run it into the PowerBook. On a PowerBook with built-in bluetooth, can I send the sound-in signal out via bluetooth? Sounds like a weekend project, to me...
medmusings: Grand Rounds XX
-
Printer Friendly|#| Trackback
All the way from Singapore......medmusings: Grand Rounds XX
Monday, February 7, 2005
More than 80 Prominent Leaders Endorse Special Health Courts
-
Printer Friendly|#| Trackback
Common Good has kicked off a national education campaign about special health care courts with a brochure titled An Urgent Call for Special Health Courts: America needs a reliable system of medical justice. (pdf also available).
I've posted about special health courts before here and support them in principle We have special courts for workman's compensation--we need special courts for malpractice issues. The proposal includes:
- Full-time judges
- Neutral experts
- Speedy processing at lower cost
- Schedule for non-economic damages
- Liberalized standard for patient recovery

Wired Magazine: Pain Management in Iraq
-
Printer Friendly|#| Trackback
The Painful Truth: The Iraq war is a new kind of hell, with more survivors - but more maimed, shattered limbs - than ever. A revolution in battlefield medicine is helping them conquer the pain.
" For soldiers evacuated from the battlefield, the advantages of nerve blocks over traditional methods of pain control are clear. The wounded troops flying in and out of Landstuhl are often in misery or a narcotized stupor, while those treated with blocks remain awake and pain-free despite massive injuries. "
A great story about how military anesthesiologists are making a big difference for our wounded.
Kaiser Daily Health Policy Report Highlights News of State Medical Malpractice Developments
-
Printer Friendly|#| Trackback
Summarizes recent developments in tort reform in Georgia, Maryland, Missouri, Nevada, North and South Carolina, and Wyoming.
[Via UK Medical News Today]
Friday, February 4, 2005
Site Update: Trackbacks Are Live
-
Printer Friendly|#| Trackback
My content management system, Conversant, now fully support Trackback as detailed here. To see the trackbacks, you'll have to look at the 'discuss' link that follows each post.
Thursday, February 3, 2005
PA State Medical Society Frivolous Lawsuit Project
-
Printer Friendly|#| Trackback
In 2004, the Pennsylvania State Medical Society began a project to support physicians who chose to countersue lawyers who brought frivolous malpractice lawsuits under the Frivolous Lawsuit Project. A recent newsletter gave the following update:
" In May of 2004, the Society settled its first frivolous case, resulting in an apology from the offending attorney and an agreement to make an undisclosed monetary payment.
The countersuit was brought by Charles Dunton, MD—a gynecological oncologist from Delaware County—against Diane Rice, Esq., of Bucks County.
Ms. Rice had filed a medical malpractice action on behalf of her client in which she accused Dr. Dunton of providing inadequate care. That action was eventually resolved in Dr. Dunton’s favor when Ms. Rice was unable to produce an expert to support her allegations.
In her apology, Ms. Rice admitted she did not obtain an opinion from a qualified medical expert prior to filing the suit... "
Wednesday, February 2, 2005
FDA Approves Generic Fentanyl Patch
-
Printer Friendly|#| Trackback
FDA Clears the Way for Generic Versions of Transdermal Patches to Treat Chronic Pain
" The Food and Drug Administration (FDA) has granted approval to Mylan Technologies, Inc., for the first generic version of Alza Corporation's Duragesic Patch (Fentanyl Transdermal System) used to treat patients suffering from severe chronic pain that cannot be managed with alternative analgesics. When applied to the skin, this patch technology delivers fentanyl, an opioid pain medication that is slowly absorbed into the body through the skin providing pain relief for up to three days (72 hours).
The agency's approval is expected to provide patients with access to a lower cost alternative of this pain management system. At the same time that FDA approved Mylan's generic product, it acted on several citizens' petitions requesting that FDA deny or delay approval of the product." "
[Via Science Blog - Science News Stories]
Medical Bills, Lost Income Due to Illness, and Bankruptcy
-
Printer Friendly|#| Trackback
Health Affairs: MarketWatch--Illness And Injury As Contributors To Bankruptcy:
" "In 2001, 1.458 million American families filed for bankruptcy. To investigate medical contributors to bankruptcy, we surveyed 1,771 personal bankruptcy filers in five federal courts and subsequently completed in-depth interviews with 931 of them. About half cited medical causes, which indicates that 1.9-2.2 million Americans (filers plus dependents) experienced medical bankruptcy. Among those whose illnesses led to bankruptcy, out-of-pocket costs average $11,854 since the start of illness; 75.7 percent had insurance at the onset of illness. Medical debtors were 42 percent more likely than other debtors to experience lapses in coverage. Even middle-class insured families often fall prey to financial catastrophe when sick." "
[Via Science Blog - Science News Stories]
Caffeine, Why Do We Love Thee?
-
Printer Friendly|#| Trackback
I spotted this National Geographics cover about my favorite drug while browsing ScienceBlog :
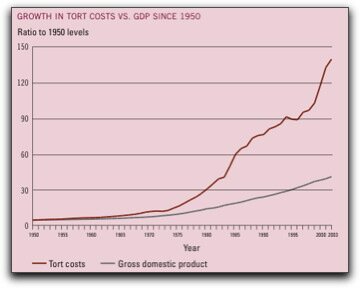
Tort System Costs
-
Printer Friendly|#| Trackback
I'm posting these data mainly so I'll be able to find them again at a later date, but others might find the numbers useful as well.
" The tort system now costs every man, woman, and child in America an average of $845 a year, almost 10 times the inflation-adjusted $91 per capita it cost in 1950. The $246 billion-a-year total comes to 2.2 percent of America's gross domestic product -- more than triple the 0.6 percent in the United Kingdom and more than double the 0.8 percent in Japan, France, and Canada. And as of 2002, only 22 percent of all tort costs went to compensate alleged victims' out-of-pocket losses; 24 percent went to pay for non-economic losses such as pain and suffering; 19 percent went to plaintiffs' lawyers; 14 percent went to defense costs; and 21 percent went to insurance overhead. "
I found this section in Better Justice: Bush's Missed Opportunity, which is quoting U.S. Tort Costs:2004 Update Trends and Findings on the Cost of the U.S. Tort System.
FactCheck: MoveOn.org Social Security Ad
-
Printer Friendly|#| Trackback
FactCheck.org got its start during the presidential election cycle and aims to "reduce the level of deception and confusion in U.S. politics." A project of the Annenberg Public Policy Center of the University of Pennsylvania, it periodically published 'fact checks' when it feels facts need to be checked (obviously). Their latest analysis is titled 'MoveOn.org Social Security Ad: Liberal group's ad falsely claims Bush plan would cut benefits 46 percent'.
" Summary
MoveOn.org launched a false TV ad in the districts of several House members, claiming through images and words that President Bush plans to cut Social Security benefits nearly in half. Showing white-haired workers lifting boxes, mopping floors, shoveling and laundering, the ad says "it won't be long before America introduces the working retirement."
Actually, Bush has said repeatedly he won't propose any cuts for those already retired, or near retirement. What MoveOn.org calls "Bush's planned Social Security benefit cuts" is actually a plan that would hold starting Social Security benefits steady in purchasing power, rather than allowing them to nearly double over the next 75 years as they are projected to do under the current benefit formula. The White House has discussed such a proposal, and may or may not adopt it when the President puts forth a detailed plan expected in late February. "
As physicians I think we need to be familiar with the facts about such major policy changes and FactCheck helps. If you like, you may sign up to receive future reports automatically.
Sunday, January 30, 2005
A Momentous Day
-
Printer Friendly|#| Trackback
The Fox News headline sums it up rather well: "A New Dawn of Democracy".
Iraq, our thoughts and prayers are with you--especially today. Let Freedom Ring!
Friday, January 28, 2005
BehindTheMedspeak: Pediatric MRIs will never be the same - thank God almighty!
-
Printer Friendly|#| Trackback
My fellow blogging anesthesiologist Book Of Joe posted BehindTheMedspeak: Pediatric MRIs will never be the same - thank God almighty! and points to new motion-correction software available for MRI's.
" "I was quite dismayed when I read on and learned that, though the software and hardware upgrades required for MRI machines to create acceptable images with a moving patient have been available for a year, 'they are not used in all hospitals and clinics.'
It is inconceivable that any institution doing MRIs wouldn't immediately buy these upgrades.
The cost of a medical negligence suit resulting from a dead or brain-damaged child is astronomical, running into the millions of dollars; it dwarfs whatever G.E.'s charging for Version 2.0.
Talk about penny-wise and pound-foolish..." "
I agree whole heartedly.

Palm Anesthesiology
-
Printer Friendly|#| Trackback
PalmSource maintains an excellent resource for anesthesiologists (thanks to Donald M. Voltz, M.D.) at Palm Anesthesiology which includes:
Software
- Medical Calculators
- Drug References
- Case-Tracking Software
- Educational Software
- Medical Billing Software
- Quality Assurance Software
- Clinical Information
E-Books
User Stories
Web Resources"
Included is some billing software I'm going to have to review...
| |
1 |
2
|
3
|
4
|
5 |
| 6 |
7
|
8
|
9 |
10
|
11 |
12
|
| 13 |
14
|
15 |
16
|
17 |
18 |
19
|
| 20 |
21 |
22 |
23 |
24 |
25 |
26 |
| 27 |
28 |
|
|
Jan Mar
|