Tuesday, December 27, 2005
Insurance Companies Trying To Curb Anesthesiologist Participation in Colonoscopies
-
Printer Friendly|#| Trackback
Propofol sedation for colonoscopies is in the news today.
Colonoscopy anesthesia popular but pricey (UPI):
"NEW YORK, Dec. 27 (UPI) -- An increasingly popular and potent anesthetic makes colonoscopies more comfortable for patients but it sharply boosts the cost, reports say."
I've given lots of propofol anesthetics for colonoscopies. Patients go off to sleep before they start, wake up when it's over and ask 'when are we going to start?' The recovery is faster and cleaner than traditional opiate/benzodiazepine sedation, allowing a center to increase the number of patients it can perform an exam on in a day.
A similar report on CNN/Money goes as far as to call the insurance company involved (Wellpoint) and ask if their executives will forego propofol. Answer?
""They'll be covered by the same clinical guidelines," the Wellpoint spokeswoman said."
I have to wonder, wouldn't the same logic apply here as applies to providing epidurals for labor? Are labor epidurals medically necessary? The American College of Gynecology, together with the American Society of Anesthesiologists has opined that "there is no other circumstance where it is considered acceptable for a person to experience untreated severe pain that is amenable to safe intervention." Ask a nurse that works with colonoscopy patients how she'd like hers done. I'll bet I know the answer.
It's not just insurance companies that are clamping down on anesthetists administering propofol to colonoscopy patients. Apparently, a group representing the gastroenterologists have asked for propofol labeling to be changed by the FDA to allow them to administer it (see safepropofol.org for more info). This same group is against Wellpoint's policy change as outlined here.
[Via Yahoo Search: anesthesia]
Saturday, December 24, 2005
Mythbusters: On Being An Organ Donor
-
Printer Friendly|#| Trackback
The Iowa Charles City Press has a nice piece titled Myth busters on being an organ donor which addresses the following myths:
"Myth: Doctors will not try to save my life if they know I want to be a donor.
Myth: People can recover from brain death.
Myth: Minorities should refuse to donate because organ distribution discriminates by race.
Myth: The rich and famous on the U.S. waiting list for organs get preferential treatment.
Myth: I am too old to donate organs and tissues.
Myth: My family will be charged for donating my organs.
Myth: Donation will disfigure my body.
Myth: Organs are sold, with enormous profits going to the medical community.
Myth: Marrow donation is painful. "
Please read and pass along...and 'yes' I'm an organ donor.
Thursday, December 22, 2005
More on why anesthesia is (or is not) safer
-
Printer Friendly|#| Trackback
Walter Olson responded to my earlier post and I feel I need to clarify what I meant. I thank him for pointing out (gently) the error of my words.
First off, I trained in the early 1990's after the advent of improved monitoring such as pulse oximetry and end tidal gas monitoring. My statement that 'overdose risk is not and was never a cause of patient morbidity and mortality in my field' was overly broad and, as Olson points out, incorrect.
The point I tried to make (though not well) was that overdose is not something we presently worry about and does not explain the apparent increase in awareness under anesthesia. What can explain it (in part) is the use of muscle paralyzing drugs (even when they are not absolutely necessary) often together with medical errors such as empty vaporizers (inhaled anesthetic delivery source), incorrectly installed vaporizers, or other human error.
Though Google turns up many hits on anesthesia and overdose, these tend to be written by non-anesthesiologists for the lay public and should not be taken as evidence that anesthetic overdoses is a cause of malpractice claims (though, admittedly, it is a term that most juries readily understand)
Walter, if you're reading this, I'd love to be able to read more about how the legal system portrays us during trials. Any pointers?
More proof: people don't change (doctors are people)
-
Printer Friendly|#| Trackback
Disciplinary Action by Medical Boards and Prior Behavior in Medical School
"Conclusions In this case-control study, disciplinary action among practicing physicians by medical boards was strongly associated with unprofessional behavior in medical school. Students with the strongest association were those who were described as irresponsible or as having diminished ability to improve their behavior. Professionalism should have a central role in medical academics and throughout one's medical career."
Another report of H5N1 resistance to Tamiflu
-
Printer Friendly|#| Trackback
NEJM Case Report: Oseltamivir Resistance during Treatment of Influenza A (H5N1) Infection [free full text]
Tight glycemic control in Type I diabetes reduces risk of cardiovascular disease
-
Printer Friendly|#| Trackback
NEJM:Intensive Diabetes Treatment and Cardiovascular Disease in Patients with Type 1 Diabetes
"Results During the mean 17 years of follow-up, 46 cardiovascular disease events occurred in 31 patients who had received intensive treatment in the DCCT, as compared with 98 events in 52 patients who had received conventional treatment. Intensive treatment reduced the risk of any cardiovascular disease event by 42 percent (95 percent confidence interval, 9 to 63 percent; P=0.02) and the risk of nonfatal myocardial infarction, stroke, or death from cardiovascular disease by 57 percent (95 percent confidence interval, 12 to 79 percent; P=0.02). The decrease in glycosylated hemoglobin values during the DCCT was significantly associated with most of the positive effects of intensive treatment on the risk of cardiovascular disease. Microalbuminuria and albuminuria were associated with a significant increase in the risk of cardiovascular disease, but differences between treatment groups remained significant (Pâ¤0.05) after adjusting for these factors."
Misconceptions about why anesthesia is safer
-
Printer Friendly|#| Trackback
Walter Olson has taught me much about the legal system as it pertains to medicine via the PointOfLaw forum. I have to take exception with a post made today however. In pointing to an article that considers whether the lessons of patient safety in anesthesiology are generalizable to other fields of medicine, he writes:
"Incidentally, because anesthesiologists are now more vigilant than ever not to court an overdose risk by giving patients any more than the minimum they need, there is apparently a rising incidence of the phenomenon of "anesthesia awareness", in which underdosed patients are actually aware of the surgery in progress and perhaps end up undergoing psychological trauma as a result. So what happens next? You guessed it."
Overdose risk is not and was never a cause of patient morbidity and mortality in my field. Second, it is not at all clear whether the 'rising incidence of the phenomenon of anesthesia awareness' is anything but a) better reporting (i.e. you don't find what you don't look for) b) realization among patients that there's something else they can sue for or c) an effort by one medical device company which makes depth of anesthesia monitors to panic hospitals and anesthesia groups into buying their product (a product which, by the way, has not been shown to decrease the incidence of awareness).
The specialty is actively engaged in evaluating this 'problem' with the same approach it has used to improve patient safety in other areas such as airway management and positioning injuries.
Tuesday, December 6, 2005
For OR Nurses: iPod 101
-
Printer Friendly|#| Trackback

"Just in time for the Holiday season Apple has posted iPod 101...[which] covers everything you might want to know about the iPod, but were afraid to ask (or perhaps didn't know you should want to ask)."
[Via TUAW]
Sunday, December 4, 2005
Sales of Impotence Drugs Fall, Defying Expectations - New York Times
-
Printer Friendly|#| Trackback
Sales of Impotence Drugs Fall, Defying Expectations - New York Times:
"Seven years after Pfizer made Viagra a cultural touchstone and commercial blockbuster, the market for impotence medicines appears to have fallen well short of what was once predicted."
[Via New York Times]
Thursday, December 1, 2005
CDC MMWR: Severe Clostridium difficile
-
Printer Friendly|#| Trackback
Severe Clostridium difficile--Associated Disease in Populations Previously at Low Risk --- Four States, 2005
Greg Pierce: Pragmatic Security
-
Printer Friendly|#| Trackback
Greg's "Pragmatic Security," for the Rest of You ;-):
" Greg has just published a very pragmatic set of instructions to help "friends and family of geeks" deal with security issues on the internet. Very good recommendations, all of them, and so I'd like to ask all of my friends and family to go check them out. He obviously spent a lot of time writing that essay, and I believe that most will find it an 'easy read'.
He admits it's not a complete solution to everyone. It's a plan to get started. I think it's a good plan.
The most important issue he left out, in my opinion, is the huge number of "phishing" email messages being sent out these days (these are attempts to trick you out of your username and password). Nobody is safe from these, many of them are just too good. I wrote up a little blurb and posted it in a reply to Greg's message, so please include it in your reading. "
[Via Truer Words - A Journal]
How do you mark a surgical site?
-
Printer Friendly|#| Trackback
The American Academy of Orthopaedic Surgeons has a policy on marking surgical sites titled Guidelines for Implementation of the Universal Protocol for the Prevention of Wrong Site, Wrong Procedure and Wrong Person Surgery. It's worth reviewing and comparing to your institutions policy. For example:
- Make the mark at or near the incision site. Do NOT mark any non-operative site(s) unless necessary for some other aspect of care.
- The mark should be unambiguous (e.g., use initials or "YES" or a line representing the proposed incision; consider that "X" may be ambiguous).
- The person performing the procedure should do the site marking.
There's much more to the guideline, but your current policies are most likely to be at variance with the above three points. One of the surgery centers I work at, for instance, marks the surgical site with an 'X'. I've explained to them that 'X' is ambiguous (does X mark the spot, or does X mark 'not this one'?) and even explained the details of a malpractice case in which marking with an X came into play. Another hospital was in the habit of marking both sides ('L' and 'R'). Also confusing. Finally, several centers have the nurse preparing the patient for surgery to mark the site. Also not a good idea.
Wednesday, November 30, 2005
NYT: Gimme an Rx! Cheerleaders Pep Up Drug Sales
-
Printer Friendly|#| Trackback
Interesting New York Times article on pharmaceutical reps:
"Exaggerated motions, exaggerated smiles, exaggerated enthusiasm - they learn those things, and they can get people to do what they want."
Approximately two dozen Kentucky cheerleaders, mostly women but a few men, have become drug reps in recent years.
While there are no statistics on how many drug representatives are former or current cheerleaders, demand for them led to the formation of an employment firm, Spirited Sales Leaders, in Memphis. It maintains a database of thousands of potential candidates."
This reminds me of the drug rep on the TV show Scrubs (played by Heather Locklear).
![]()
Friday, November 25, 2005
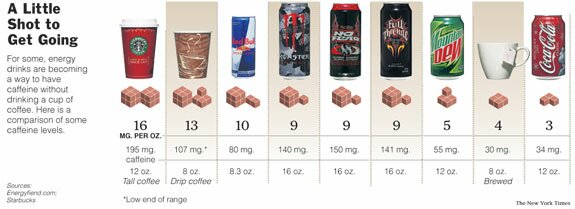
How much caffeine does that drink have?
-
Printer Friendly|#| Trackback
I've written before about caffeine addiction in surgical patients. In recent years there's been an explosion of caffeine-containing beverages. Having some idea of the caffeine content of the major ones can help you choose an appropriate dose.
The Energy Fiend web site has a nice Caffeine Database. I found it via a recent NYT article.
Thursday, November 24, 2005
NEJM: The Origins of Pandemic Influenza--Lessons from the 1918 Virus
-
Printer Friendly|#| Trackback
The Origins of Pandemic Influenza--Lessons from the 1918 Virus [free full text]
"...monitoring of the sequences of viruses isolated in instances of bird-to-human transmission for genetic changes in key regions may enable us to track viruses years before they develop the capacity to replicate with high efficiency in humans. Knowledge of the genetic sequences of influenza viruses that predate the 1918 pandemic would be extremely helpful in determining the events that may lead to the adaptation of avian viruses to humans before the occurrence of pandemic influenza. We could then conduct worldwide surveillance for similar events involving contemporary avian viruses. "
How To: Awake Fiberoptic Intubation
-
Printer Friendly|#| Trackback
This definitely falls in the "don't try this at home" category, but if this technique is different than the one you use, give it a try. It will surely result in a net gain in style points.
How To Do An Awake Fiberoptic Intubation
Technorati Tags: Anesthesia
Wednesday, November 23, 2005
C-section rate in USA reaches 29.1% in 2004
-
Printer Friendly|#| Trackback
" Despite the evidence of risks associated with cesarean section, the rate of birth by cesarean section in 2004 in the USA registered at 29.1 percent, the highest ever recorded. According to the Centers for Disease Control and Prevention (CDC) in a recent report, this figure is an 8 percent increase from 2003, and a 41 percent increase since 1996. "
One of the OB practices at our hospital has a policy that they will not do vaginal births after C-section (VBAC)...largely due to concern about lawsuits.
[Via UK Medical News Today]
MMWR Available Via Really Simple Syndication (RSS) Feeds
-
Printer Friendly|#| Trackback
"MMWR now offers RSS feeds, a free, automated method to receive all MMWR publications. Through RSS, new reports and publications are fed to your desktop or browser-based news reader when they are posted online. Headlines are presented in the RSS feeds, with links to the full reports and publications on the MMWR website. RSS feeds to MMWR publications are available at http://www.cdc.gov/mmwr/rss/rss.html"
[CDC]
| |
1
|
2 |
3 |
|
4
|
5 |
6
|
7 |
8 |
9 |
10 |
| 11 |
12 |
13 |
14 |
15 |
16 |
17 |
| 18 |
19 |
20 |
21 |
22
|
23 |
24
|
| 25 |
26 |
27 |
28
|
29 |
30 |
31 |
|
Nov Jan
|